Nutrition is an important part of the health of all children, but it is especially important for Children with Cancer. It is therefore of vital importance that you learn about your child’s nutritional needs and how cancer and its treatment may affect them.
Eating the right kinds of foods before, during, and after treatment can help a child feel better and stay stronger. It is also important so that the Child with Cancer can cope with treatment side effects that might affect how well they can eat.
Children with Cancer need protein, carbohydrates, fat, water, vitamins, and minerals. A dietitian can help you understand your child’s specific needs and develop an eating plan.
Proteins
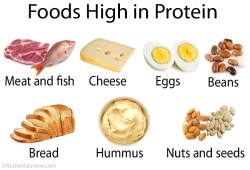 The human body uses protein to grow; repair tissues; and to maintain the skin, blood cells, immune system, and the lining of the digestive tract.
The human body uses protein to grow; repair tissues; and to maintain the skin, blood cells, immune system, and the lining of the digestive tract.
Children with Cancer who do not get sufficient protein might break down their muscle for the fuel their bodies need, which will result in them taking longer to recover from any illness; this can also lower their resistance to infection. After a child has surgery, chemotherapy, or radiation therapy treatments,he or she may require additional protein to heal tissues and help prevent infection.
Protein is also key to a child’s growth and development. During illness, a child’s need for protein goes up.
Good sources of protein include poultry, fish, eggs, lean red meat, dairy products, nuts and nut butters, dried beans, peas and lentils, and soya.
Carbohydrates
 Carbohydrates are the body’s major source of energy – they give the body the fuel (calories) it needs for physical activity and proper organ function.
Carbohydrates are the body’s major source of energy – they give the body the fuel (calories) it needs for physical activity and proper organ function.
The amount of calories a child needs depends on their age, size, and level of physical activity. Healthy infants, children, and adolescents need more calories per kilogram than adults to support growth and development.
Children with Cancer may require even more calories for tissue healing and energy. A Child with Cancer may need anywhere from 20% to 90% more calories than a healthy child.
The best sources of carbohydrates are fruits, vegetables, and whole grains, and they provide the body’s cells with the fibre, vitamins and minerals, and phytonutrients required.
Whole grains or foods made from whole grains contain all the essential components and naturally occurring nutrients of the entire grain seed.
Whole grains are found in cereals, breads, flours, and crackers. Some whole grains can be used as side dishes or part of an entreé. When choosing a whole-grain product, look for the words “whole grain,” “stone ground,” “whole ground,” “whole-wheat flour,” “whole-oat flour,” or “whole-rye flour.”
Fibre is the part of plant foods that, most of the time, the body cannot digest. There are 2 types of fibre:
- Insoluble fibre takes up space in the intestine, and speeds up the passage of food waste out of the body.
- Soluble fibre binds with water in the stool to help keep the stool soft while it slows down digestion.
Other sources of carbohydrates include bread, potatoes, rice, spaghetti, pasta, cereals, dried beans, corn, peas, and beans. These carbohydrate foods also contain B vitamins and fibre. Sweets (desserts, sweets and fizzy drinks) give your child carbohydrates, but very few other nutrients.
Fats
 Fats play an important role in nutrition. Fats and oils consist of fatty acids and serve as a rich source of energy (calories) for the body, which breaks down fats and uses them to store energy, insulate body tissues, and transport certain vitamins through the blood.
Fats play an important role in nutrition. Fats and oils consist of fatty acids and serve as a rich source of energy (calories) for the body, which breaks down fats and uses them to store energy, insulate body tissues, and transport certain vitamins through the blood.
Unsaturated fats (monounsaturated and polyunsaturated) should be chosen more often than saturated fats or trans fats:
- Monounsaturated fats are found mainly in vegetable oils such as olive, canola, and peanut oils. They are liquid at room temperature.
- Polyunsaturated fats are found mainly in vegetable oils such as safflower, sunflower, corn, and flaxseed oils. They are also the main fats found in seafood. They are liquid or soft at room temperature.
Saturated fats (or saturated fatty acids) are mainly found in animal sources, such as meat and poultry, whole or reduced-fat milk, cheese, and butter. Some vegetable oils like coconut oil, palm kernel oil, and palm oil are saturated. Saturated fats are usually solid at room temperature.
Trans-fatty acids are formed when vegetable oils are processed into margarine or shortening. Sources of trans fats include snack foods and baked goods made with partially hydrogenated vegetable oil or vegetable shortening. Trans fats also are found naturally in some animal products, such as dairy products.
Certain fatty acids, such as linoleic acid and alpha-linolenic acid, are called essential fatty acids. They are needed to build cells and make hormones, but because the body cannot make them, we must get them from foods. Soybean, canola, and walnut oils are good sources of essential fatty acids.
Water
 The human body is made up of between 70% – 85% water (the percentage gets less as one gets older), and there is water in every single cell in the human body.
The human body is made up of between 70% – 85% water (the percentage gets less as one gets older), and there is water in every single cell in the human body.
If your child does not take in enough fluids or loses fluids from vomiting or diarrhoea without replacing them, he or she may become dehydrated. If this happens, the fluids and minerals that help keep the body working can become dangerously out of balance.
Children can get some of the required water from foods, especially fruits and vegetables, but they need liquids to be sure that all the body cells get the fluid they need. The amount of fluid a child needs depends on his or her size and how much liquid he/she is losing. If he or she is vomiting or has diarrhoea, they need to drink more fluids, especially water. All liquids (soups, milk, even ice cream and gelatine) do count toward your child’s fluid goals, but the majority should be made up of water.
Indications of dehydration include a dry mouth, headaches, fatigue, dark coloured urine, listlessness, and dizziness. An easy way to check if your child is dehydrated is to lightly pinch up the skin over the breast bone; if the skin does not return to normal and stays raised, your child may be dehydrated.
Vitamins & Minerals
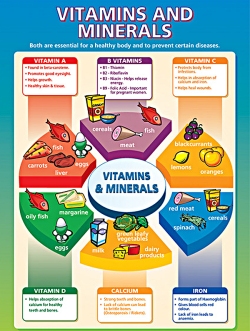 The body needs small amounts of vitamins and minerals for normal growth and development, and to help it function properly. Vitamins and minerals also help the body use the energy (calories) it gets from food.
The body needs small amounts of vitamins and minerals for normal growth and development, and to help it function properly. Vitamins and minerals also help the body use the energy (calories) it gets from food.
Children who eat a balanced diet usually get plenty of vitamins and minerals. Studies have shown, however, that even healthy children often do not get sufficient calcium and vitamin D, which are vital for bone growth. Some of the drugs used to treat cancer can lower calcium and vitamin D levels, so your child may need to take additional amounts.
It may be difficult for a Child getting Cancer Treatment to eat a balanced diet. Common treatment side effects, like nausea, vomiting, and mouth sores (mucositis) can make it hard to eat.
The doctor may recommend a daily multivitamin while your child is being treated, but multivitamins do not replace eating enough calories and protein. Never give your child any form of multivitamin, minerals, or supplement without speaking to their doctor first, as some of them might interfere with their cancer treatment.
We will be continuing to post more about Nutrition in Childhood Cancer as well as some great recipes to help ensure that your child gets the nutrition they require as we go, some come back regularly to view the most updated information.
Source: Little Fighters Cancer Trust | Author: LFCT




 Up until now, drug companies have been free to decide whether to pursue treatments for paediatric cancers as part of their work on adult cancers or not, and this has led to a minimal amount of new drugs specifically for paediatric cancers being developed.
Up until now, drug companies have been free to decide whether to pursue treatments for paediatric cancers as part of their work on adult cancers or not, and this has led to a minimal amount of new drugs specifically for paediatric cancers being developed. said Jorge Luis Lopez, a Miami attorney who sits on the board of the American Cancer Society. “We urge Donald Trump to sign this legislation into law and unleash American innovation and creativity for the health and well-being of all our children.”
said Jorge Luis Lopez, a Miami attorney who sits on the board of the American Cancer Society. “We urge Donald Trump to sign this legislation into law and unleash American innovation and creativity for the health and well-being of all our children.”
Most Commented